Pulmonary embolism (PE)
it is not complete but do include key points that we need to know to work in ward.
pathophysio:
- it results from DVT - venous thromboembolism
- venous stasis, endothelial injury and hypercoagulability.
bridging:
- egfr>30: s/c clexane BD
- egFR 15-30 - s/c clexane OD
- eGFR <15 - IVI heparin (kena monitor coag 6 hourly)
- Warfarin affects the APTT & PT value
- Clexane - APTT (to help INR reaches the aim faster)
- Aim INR 2-3, once INR >2, off clexane, bridging complete
4th day start adjusting dose base on INR
- pharmacist has special counsellor or booklet for the patient to understand the use of warfarin. with constant follow up and also diet suggestions (no green leafy veges)


Investigations(Ix):
1. ECG :look for ST changes S1Q3T3
- deep S wave in lead I, Q wave in lead 3, T inversion in lead 3
- ST depression, RBBB
- P. pulmonale

2. blood Ix: trop t and ck stat
3. basic supportive tx: HFM, transfer to acute bed
request for :
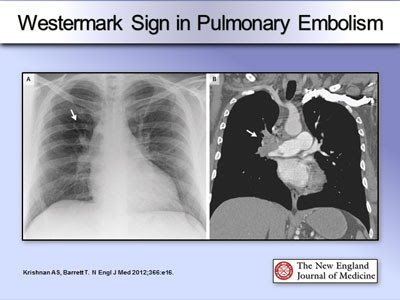
- CXR : hamptoms hump: wedgemark sign, westermark sign: pulmonary oligaemia in the affected segment


- CTPA : thrombi within pulmonary

https://epos.myesr.org/poster/esr/ecr2020/C-04154
- for those who have clot in the past, and have a previous episode before, or those who has acute kidney damage/ckd.
- clear cxr
- ultrasound for lower limb: to rule out lower limb DVT due to long sitting/surgery...
- start DAPT
4. echo:
- look for RV dilation and hypokinesia. - acute rv failure--> increase afterload, rv cannot unload sufficiently causing rv dilated. impinge on LV cause LV to decrease output and supply to CA
- it increases o2 demand which CA could not meet, results in ischemia and necrosis
- it increases o2 demand which CA could not meet, results in ischemia and necrosis
MASSIVE PE:
HYPOTENSION BP<50 for at least >15MINUTES, HR <40 - usually with evidence of MI and hyocardial dysfunction
Well's score for PE
low<2, mid 2-6, high >6
1. clinical signs of DVT -3
2. previous surgery / long traveeling>4hrs -1.5
3. previous DVT and PE- 1.5
4. HR>100 - 1.5
5. other diagnosis seem less likely -3
6.hemoptysis -1
7. cancer -1
1. clinical signs of DVT -3
2. previous surgery / long traveeling>4hrs -1.5
3. previous DVT and PE- 1.5
4. HR>100 - 1.5
5. other diagnosis seem less likely -3
6.hemoptysis -1
7. cancer -1

Management (Mx):
anticoagulant- without hypotension: LWMH, fonda/ DOACS- unstable/ bleeding: parental anticoag 5-10d, switch to warfarin overlap 3-7d before discontinue heparin when INR >2 for >2d- continue anticoag for 3-6months
thrombolytic therapy:
STK 25mu if pt high risk massive PE/ with cardiopulmonary arrest.
other mx:
1. rivaroxaban 15mg BD for 21d then 20mg OD2. dabigatran (expensive)
Reference:
No comments:
Post a Comment