Criteria mentioned
if you cant remember can search https://www.mdcalc.com/ for auto calculation as well.
 |
| commonly used criteria in ward |
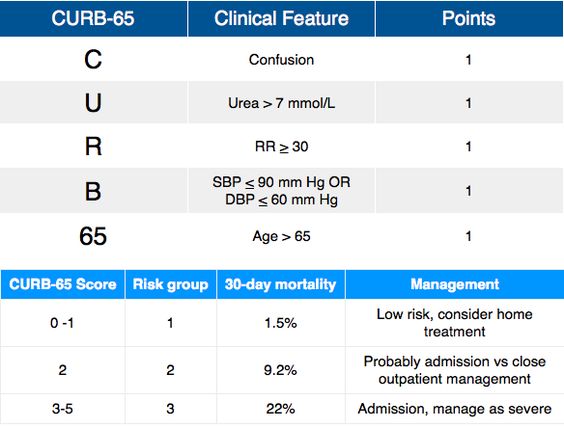
Pneumonia - CURB 65
Confusion, urea>7, RR>30, BP<90/60, >65years old
Stroke risk - CHADS VASC
- chronic heart failure-1, HTN-1,>75 years old-2, age 65-74 - 1, DMT2-1, stroke-2, vascular disease-1, female-1
-0: no antocoagulation needed, 1 : either no or with anti coag therapy, >2: oral anticoag theraphy recommended

Risk of bleed - HAS BLED
- HTN, Abnormal renal and liver fx(1 point each), stroke, bleeding, labile INR, Elderly >65, drugs or alcohol
- 0-2 low risk bleeding, >3 high risk bleeding, HTN : SBP>160

Peritoneal fluid - SAAG (serum to ascites albumin gradient)
serum albumin - albumin in ascitic fluid
- more useful than the protein based exudate/transudate concept.
>1.1 transudate/ indicates portal HTN (budd chiari, cirrhosis), <1.1 is exudate: look for inflammatory/neoplastic causes
Pleural fluid - Light's criteria
- to distinguish transudate or exudates
LDH/pleural fluid LDH, pleural fluid protein/ serum protein, pleural fluid/ serum LDH

Myocardial infarction - TIMI / KILIP
- thrombolysis in MI
TIMI: >65yo, >3risk factor of CAD, known CAD(stenosis>50%), ASA used past 7d
presented with recent chest pain<24hours, increase cardiac marker, ST deviation>0.5mm
- 0-2 low risk, 3-5 intermediate risk, 6-7 high risk

KILLIP: I: no congestion sign, II: with S3 basal rales, increase JVPIII: acute pulmonary edema, IV: with cardiogenic shock (bp<90/60, oliguria, cyanosis, impaired mental status)

NYHA: I: no symptoms and no limitations , II: mild symptoms and slight limitation III: significant limitation , comfortable at rest IV: severe limitation, Sx even at rest

PEmbolism Wells score
clinical signs of dvt, no alternate dx, hr>100, immobilise>3d, previous dvt/pe, malignancy, hemoptysis - 7 items

DVT well score: <2 DVT unlikely
- active cancer, paralysis, recent bedridden>3mth, localised tenderness, leg swollen, calf swelling, pitting edema on symptomatic leg, collateral superficial vein, previous dvt, alternate dx is at lease as likely as dvt (-2)

Padua risk assessment:

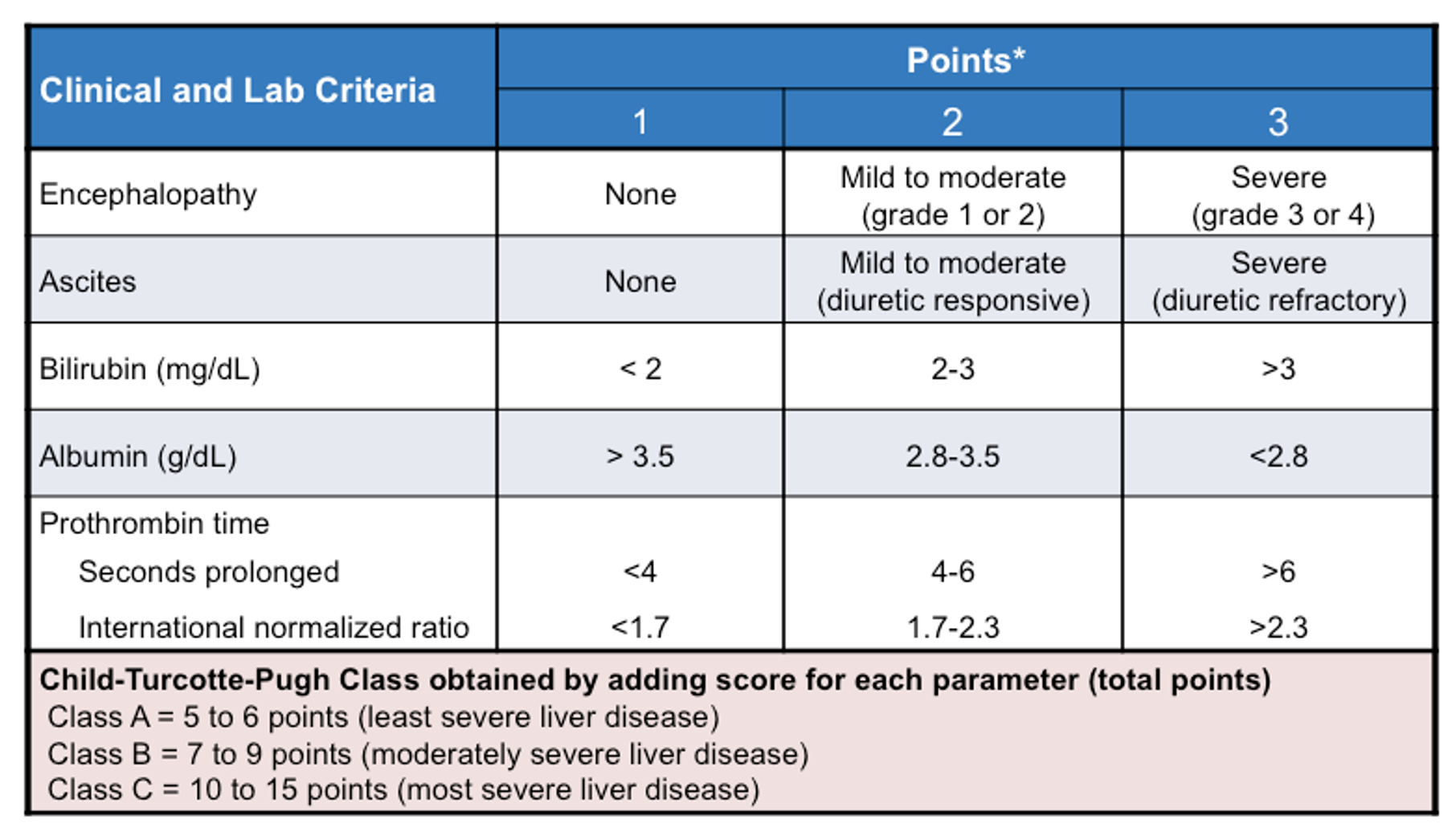
Liver cirrhosis - Child Pugh score
encephalopathy, INR>2/<1.9, Alb <2.8/>4, TB: >3.5/<1.8
10-15 child pugh C, 6-9 child pugh B, 1-5 child pugh A
GOLD ( COPD staging)
I-early, II-moderate, III-severe, IV-very severe


MMRC ( dyspnea severity)
0-4

Duke's criteria ( diagnose IE)
- 2major and 5 minor
- tp dx: at least 1major 1minor/ 5minor
- 2major: positive blood culture, endocardial involvement: echo positive for IE
-5 minor: fever>38, vascular phenomena, history of IVDU, immunologic phenomena, microbiological evidence
- 1 that rule them all is when Coxiella burnetii or antiphase I IgG antibody titer>1:800

Thyroid storm - Burch Wartofsky point scale

BWPS:>45 - definitive of thyroid storm, 25-44 clinical judgement needed

Mx: PTU 500-1000mg loading, then 250mg 4-6hourly - if cant give MMI 60-80mg/d
- high dose of IV HCT 100mg, 6hrly dexamethasone 2mg, 6hrly (to inhibit both thyroid
hormone synthesis and peripheral conversion of T4 to T3)
Obstructive sleep apnea - STOP-BANG
- snoring, tiredness, observed apnea, high bp, bmi, age>50, neck circumference, male

ICH (mortality rate in ICB)
Intracerebral hemorrhage - GCS, age>80, location, ICH volume>30, intraventricular blood

NIHSS (assessment of stroke severity)
national institute of health stroke scale score: 11 item
LOC, gaze, visual, facial palsy, motor arm /leg, sensory, language, dysarthria, extinction n inattention
Framingham Risk Score (risk of MI)
- Age, HDL, FLP, BP, DM, smoker,

qSOFA (quick septic shock assessment)

- q sequential organ failure assessment

ABCD2 score ( stroke risk after TIA)

EGSYS (identify cardiac syncope)

- evaluation of guidelines in syncope study
 |
| EGSYS |
9 KPI for stroke patient
 |
| 9 KPI for stroke |
Others:
1.Oxfordshire classification for stroke
2. CCS score ( severity of exertional angina)
3. Mayo DAI score ( severity of ulcerative colitis)
4. SLICC criteria ( diagnosis of SLE)

5. MELD score ( liver transplant assessment)
6. APRI score ( likelihood of9 fibrosis and cirrhosis in patients with Hepatitis C)
7. Lee index ( risk of perioperative cardiac events)
8. Epworth sleepiness scale ( to diagnose OSA)
9. Mehran risk score (prediction of CIN)

10. Rheumatic fever (JONES criteria):
throat cultures: GABHS or elevated anti-streptolysin O titers + 2 major / 1major+2minor

No comments:
Post a Comment