Necrotising Fasciitis vs Gangrene


** REMEMBER TO ALWAYS DO RESUSCITATION FIRST PRIOR OTHER MANAGEMENT (ABX, ANALGESICS, DM CONTROL)
Indication for amputation: 3D's
🐣 Dying / diseased bone - PVD, infection, gangrene, trauma
🐣 Dangerous - lethal sepsis, malignant
🐣 Damn nuisance - gas gangrene, crush syndrome, severe malformation
Sample Xray

Gas shadows seen extending from the foot up to upper calf
Doppler
Usually medical officer will ask for a doppler done and also ABSI.
So try to get your doppler right.
There are three spots that we must check : the Dorsalis Pedis Artery (DPA), Posterior Tibial Artery (PTA) and Brachial



Normal ABSI: 1.0-1.3 Normal wave: Triphasic
ABSI 0.5-0.9: moderate to severe
ABSI >1.3: common in DM (may have severe calcifications)
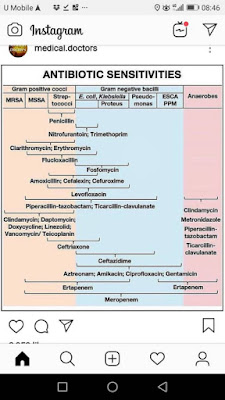
Antibiotics:
For NF: commonly polymicrobial bacteria can be seen.
- - IV Tazocin 4.5g QID (consist of piperacillin and tazobactem)
- - IV clindamycin 600-900mg TDS
- inhibitor of protein synthesis and protein m synthesis
- effective for gram +ve
- or Cefotaxime + metronidazole
- - unasyn (beta lactam, inhibiting bacterial cell wall synthesis)
- - ciprofloxacin : covers gram negative
Reference:
- WD: wound debridement
- h/o : history of
- DM : Diabetes Mellitus
- DFU : Diabetes Foot Ulcer
- ABSI : Ankle Brachial Index
No comments:
Post a Comment