Here is the summary of IOL and more information do scroll down to understand further details.

Notes:- IOL : Induction Of Labor
- GDM: Gestational Diabetes Mellitus
- PROM: Premature Rupture of Membrane
- IUD: Intrauterine Death
- IUGR: Intrauterine Growth Restriction
- LGA: Large Gestational Age
- NRVE: Next Review Vaginal Examination
- NRC: Next Review Contraction
- LSCS: lower segment caesarean Section
- IOL : Induction Of Labor
- GDM: Gestational Diabetes Mellitus
- PROM: Premature Rupture of Membrane
- IUD: Intrauterine Death
- IUGR: Intrauterine Growth Restriction
- LGA: Large Gestational Age
- NRVE: Next Review Vaginal Examination
- NRC: Next Review Contraction
- LSCS: lower segment caesarean Section
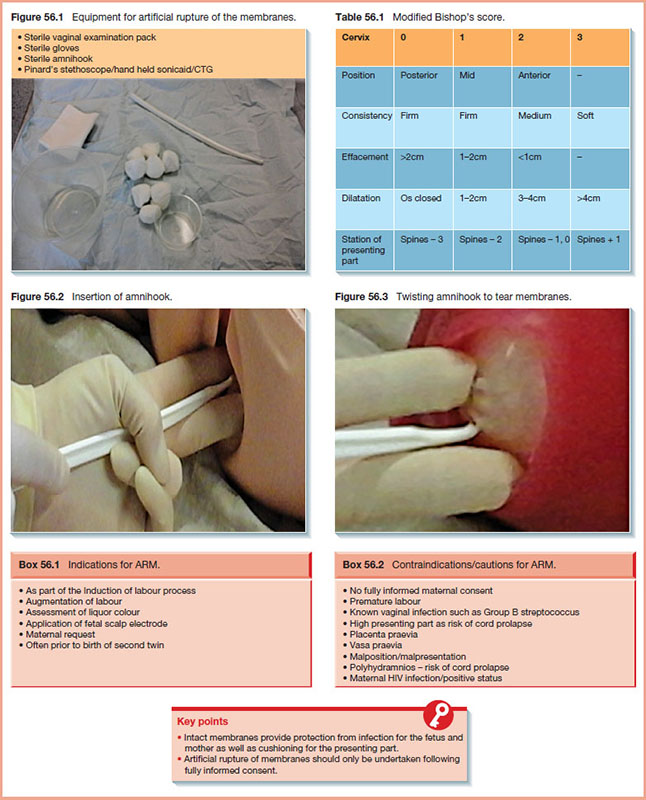
Bishop score

Balloon Device
Inflated bulb of a Foley catheter exerts pressure to the internal os of the cervix which then stretches the lower uterine segment and stimulates release of prostaglandin (PG)
Contraindicated in patients with low-lying placenta
The catheter is left in place until it falls out spontaneously/24 hours have elapsed
Pharmacological approach

Artificial Rupture of Membrane
- one of the ways of induction of labor (IOL), usually to speed up the process of labor
- only been done when cervix is dilated to >4cm or > 3cm if indicated
- and baby's head firmly decended to the pelvis.
Contraindication:
1. Bishop score<6
2. breech
3. grandmultipara
4. preterm
5. high presenting head
6. polyhydramnious - if rupture is needed: need to have controlled ARM
- where assistant is needed to control the baby's position to avoid baby from changing position
Risk:
1. cord prolapse: if the baby head is not engaged well, and membrane rupture causing the cord to slip down below the baby's head.
2. Sepsis: when the labor time is prolonged
3. Failure of induction
4. increase risk of fetal distress

Before you start ARM procedure, always remember to check
- Patient's name, and registration number
- confirm Antenatal history
- Are they indicated for ARM?
- or any contraindications
- check if any oligohydramnious / polyhydramnious - as baby could change position if not stabilised
- How is the position of the mother and Baby?
- Ensure there is an IV line set already with IV drip
- Vaginal Examination: any cord/ placenta
- Cx and Os dilation, Station
- Ensure mother is not having contraction when you wanted to rupture the membrane
- only rupture when there is no contraction
- to avoid causing chorioamnionitis (acute inflammation of the membranes and chorion of the placenta, typically due to ascending polymicrobial bacterial infection in the setting of membrane rupture.)

Post ARM
- monitor mother's
- vital sign
- contraction
- progress of labor
- Vaginal examination 4hrly.
- time contraction (NextReview of Contraction): 2hrly
- baby's fetal heart rate
References:
No comments:
Post a Comment